Hello all! Welcome back to the Mosaic Diagnostics blog. Today’s installment will focus on some of the more confounding markers of the Organic Acid Test (OAT). The ketone and fatty acid oxidation markers seem to cause some uncertainty. Here we aim to understand the biochemistry behind this set of markers and what causes them to be elevated.

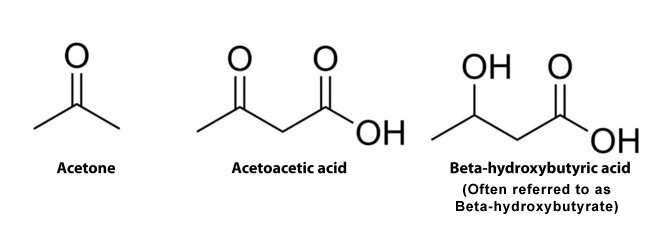
Markers 43 and 44, acetoacetic acid and 3-hydroxybutyric acid respectively, are ketones. Ketones in themselves are breakdown products of fatty acid metabolism. When fat is used as an energy source it is converted into ketones in the liver by a process called ketogenesis. First, free fatty acids are released and converted into acetyl CoA, via beta oxidation in the liver’s mitochondria. Two of these acetyl-CoA molecules are then combined to make ketone bodies. These ketones then leave the liver and make their way to extrahepatic tissues via the bloodstream. In the cell, ketones are broken down back into acetyl CoA, via beta oxidation, for entrance into the Citric Acid Cycle. This process is always occurring on some level in the body.
In times of elevated urinary ketones this means that beta oxidation has been upregulated, as it is our primary pathway for fatty acid metabolism. In times of increased ketogenesis, more ketones are being formed and the turnover into acetyl CoA is not keeping up with ketone production. This is due to more ketones being produced than energy needed by the body, so ketones will build up and be excreted into the urine, leading to an increase in markers 43 and 44.

There are many biologic processes that lead to this phenomenon. Some common, more purposeful, processes are mainly common dietary changes. Ketogenic diets, low carb inspired diets, and also 12-18 hour fasting are all purposeful reasons for elevated ketones. Due to the surge in low carb eating and intermittent fasting, elevations in markers 43 and 44 are common. These markers can come in handy when monitoring someone on a keto or low carb eating plan. Whenever elevations are present it is a good idea to rule out dietary changes that could impact these values.
Other, more concerning reasons for these elevations in ketones include a myriad of processes. A common reason in those with G.I. upset is vomiting and diarrhea. The purging associated with these processes leads to an increase in ketogenesis as all sources of energy are being purged and fat must be used to continue biological processes. B12 deficiency is another cause of increased ketones. Due to the requirement of B12 as a cofactor for the enzyme methylmalonyl CoA reductase needed for beta oxidation of odd chain fatty acids, B12 deficiency can cause a buildup of urinary ketones. This enzyme converts methylmalonyl CoA to succinyl CoA for the incorporation into the CAC or gluconeogenesis for ATP production. Due to a buildup of methylmalonyl CoA and a decrease in succinyl CoA, the body upregulates ketogenesis to meet our energy needs. To determine B12 deficiency is a possible cause be sure to review marker 50, methylmalonic acid.
Another possibility is an eating disorder. This could be due to diagnosed or undiagnosed anorexia or bulimia. When the system is malnourished or going through a prolonged fast or purging, the body will upregulate fatty acid metabolism and ketogenesis for adequate energy production. Situations where the body cannot utilize carbohydrates for energy production will also lead to increased ketones. One common cause is insulin resistance. In times of blood sugar dysregulation, due to a lack of insulin production or insulin resistance, the body must rely on fat metabolism to make ATP. This leads to an increase in ketones in the urine. Potentially this leads to a life-threatening state of ketoacidosis. In an individual consuming carbs in their diet, but also has ketones elevated, insulin resistance should be ruled out. This phenomenon can happen in relation to diabetes type 1 and type 2. An additional culprit for urinary ketones is fungal overgrowth. Fungus can readily absorb and metabolize carbohydrates. When in our intestinal tract, these organisms come into contact with the carbs we eat. In an overgrowth, more fungus is present and can potentially absorb and metabolize enough of the carbs eaten to switch the body into glycogenolysis and eventually ketogenesis. In absence of a low carb diet, all possible causes of elevation should be assessed.

The rest of the markers in this section are Fatty Acid Oxidation Markers. 45-49, ethylmalonic, methylsuccinic, adipic, suberic, and sebacic respectively, are known as dicarboxylic acids. These are the breakdown products of a secondary process for fatty acid metabolism called omega fatty acid oxidation. This process differs from beta oxidation in many ways. Omega oxidation is completed in the smooth ER of the liver and kidneys instead of the mitochondria as beta oxidation. Fats that are long and medium chain, having 10-12 carbons, undergo omega fatty acid oxidation and dicarboxylic acids are the end product. This process is an added support to our primary beta oxidation. In addition to dicarboxylic acids being produced, succinyl CoA is also produced for incorporation into the CAC and gluconeogenesis.
Omega Oxidation is upregulated in times of overwhelmed beta oxidation, increased fatty acids outside of the mitochondria, and certain dietary changes. In times of slight elevations in these markers, check the dietary intake of the client. In times of increased long chain and medium chain fat intake from omega rich fats, fish or cod liver oil supplements, and coconut oil or MCT oil, we can see noticeable increases in these markers. This is due to upregulation of beta oxidation for medium chain fats and the need for omega oxidation to upregulate to process the fats in the diet. Other dietary changes that can cause expected elevations include increased intake of “junk” foods and gelatin. These foods can have adipic acid as an additive that can be expressed in this marker’s elevation. In a state of fasting, the body will use both primary and secondary metabolism processes for ATP production and suberic acid is commonly produced.
Additional factors that lead to elevations here will include any reason that upregulates ketogenesis or blocks beta oxidation as mentioned above. These factors upregulate the body’s use of fats and this secondary pathway has to kick in to support the state of metabolism. Furthermore, certain nutritional deficiencies will block beta oxidation. As mentioned, B12 deficiency will block the production of succinyl CoA from odd chain fatty acids leading to increased ketones production and omega fatty acid oxidation to support energy needs.
Riboflavin Deficiency is another possibility. Vitamin B2 is a required cofactor for beta oxidation. It is required for a key process of acyl CoA dehydrogenation that begins each cycle of beta oxidation. In a deficient state, beta oxidation cannot begin and fatty acids have to be metabolized through our secondary process. There are also genetic factors that could increase these markers. Increases would be extremely significant and often found in infancy. These causes are known as Multiple acyl-CoA dehydrogenase deficiency (MADD) also known as glutaric aciduria type 2 and Medium chain acyl-CoA dehydrogenase deficiency (MCAD). In MADD, the person doesn’t have the adequate amounts of various acyl-CoA dehydrogenase enzymes. While MCAD is a deficiency of just the one enzyme. These are defects in fatty acid metabolism disorders. In both conditions, high dose riboflavin is warranted for support along with l-carnitine supplementation coupled with a low fat high, carb diet.
L-Carnitine is a common amino acid described regarding fatty acid metabolism. Due to the process of beta oxidation being in the mitochondria of the cell, the fatty acids have to get to the mitochondria to be processed. Short chain and medium chain fatty acids can pass the mitochondrial membrane, but it is impermeable to long chain fatty acids. Due to the impermeability, the Carnitine Shuttle is used to shuttle long chain fatty acids into the mitochondria for beta oxidation. In times of protein malnutrition or maldigestion, there is less carnitine, lysine, and methionine. Lysine and methionine are amino acids that our system can biologically synthesized into carnitine. When carnitine is deficient due to diet, genetic carnitine deficiency, times of stress, or maldigestion, long fatty acids cannot get into the mitochondria. This will upregulate omega fatty acid oxidation happening outside of the mitochondria. In any case of upregulated dicarboxylic acids, l-carnitine is an appropriate support.
In the understanding of the ketone and fatty acid oxidation section of the OAT, there are many possibilities as to why these markers are elevated. We must evaluate if it is due to nutritional deficiencies, dietary changes, overgrowths, or genetic alterations. These are the questions we as practitioners must ask ourselves