
Mosaic EDGE (formerly GPL Academy) has been educating practitioners for over 15 years on how to help patients heal through cutting-edge testing, research and protocols. In our recent 2-Day OAT+TOX Workshop, speakers focused on the epidemic of environmental toxin exposure, from the many chemicals we encounter every day to mycotoxins released from mold. Attendees learned about many common environmental pollutants from the 173 chemicals tested by the GPL-TOX Profile.
The following Q+A is a grouping of responses from a distinguished pool of speakers who participated in the OAT+TOX Workshop with his own unique topics and lectures as labeled.
The material contained within this article is not intended to replace the services and/or medical advice of a licensed healthcare practitioner, nor is it meant to encourage diagnosis and treatment of disease. It is for educational purposes only. Any application of suggestions set forth in the following portions of this article is at the reader’s discretion and sole risk. Implementation or experimentation with any supplements, herbs, dietary changes, medications, and/or lifestyle changes, etc., is done so at your sole risk and responsibility.
Managing the Complex Patient: Using the GPL-TOX and OAT in Clinical Practice
Q: What cutoff is ‘Lots” on an ERMI?
A: I typically start paying attention if the number is over 2; but in my state (Michigan), many houses are over 2. The ERMI score also does not take into account how moldy the house is in general, only the difference between toxin producing mold and non-toxin producing mold. I will use the mold numbers to calculate a HERSMI Score. If it is over 16, the house is a problem. 12-16 might be a problem if the person is sensitive.
Q: Can mycotoxins cause a progressive pulmonary fibrosis?
A: I think that anything that causes consistent immune activation (like mold toxins) can cause pulmonary fibrosis.
Q: How about triphala? Ayurvedic herb that helps with constipation and detoxifier, antioxidant and more..
A: I frequently use Triphala to help with constipation. I don’t use is it as a detoxifier/antioxidant/etc—I think there are better options for that.
Q: Are you familiar with phenomenal AIRE? It produces ions? Is this ozone?
A: It is not ozone, but it incidentally generates ozone from room air. The idea behind an ionizer is to charge particles so they stick to each other and surfaces. The energy needed to create the ions can also create ozone from the oxygen in the air. I am not a fan.
It is said to join particles to bond together known as agglomeration.
Q: What are your thoughts regarding treating mold with thermal fogging with a solution like BioBalance vs. treating with ozone generator?
A: I think ozonation is probably the most effective way of treating mold after you have removed the obvious contamination (this won’t get mold off of wood joists or rafters because it won’t penetrate the wood deeply enough) with other techniques. This requires that people are out of the building and requires an industrial strength, whole house ozonator.
Q: In a patient with Gilbert’s, what precautions are needed?
A: The issue with Gilbert’s is that they will be more susceptible to certain environmental toxins. Supporting glutathione (NAC, ALA, liposomal glutathione supplements, Setria) can help with glucuronidation (the problem with Gilbert’s).
Q: I also live in Michigan. What water filter do you find works well with our water?
A: Every water system will have different issues. I am on a well. I have completely different issues than someone that is on Detroit City water. I use the Zero Water filter—this is a pour through, multi-stage system that removes almost everything. My biggest problem is iron and bacteria—not any issues with other water supplies. This system will also remove chlorine and fluoride and heavy metals. Most of the time, a combination charcoal/reverse osmosis water filtration system works for most things, but does not remove all the thyroid.
Q: Can you just take ox bile with binders so patients have more time flexibility? Some must take meds before eating.
A: Yes. You can take them together.
Q: Patients with severe MCS that have such a hard time taking ANY med/supplement…where do you start with mold or mycotoxin treatment? Slow small amounts of binder until tolerating?
A: First, I will start with supportive supplements (like vitamin C) before I start with detox supplements. Then, I will start with a single binder (not a combination) at low dose and work my way up. Many of the symptoms MCS patients have are related to histamine, so I also tend to start with things like luteolin (and quercetin if they are not sensitive to salicylate).
Q: Is Cholestyramine constipating?
A: It is almost always constipating. I always start something (like magnesium citrate or sodium ascorbate) to help with the constipation.
Q: Do you have any protocols for people to detox from the CV injections and their injuries?
A: I assume you are referring to the COVID vaccines—check out the FLCCC.org website. They have a protocol for long-haul COVID. It works for most vaccine injuries. Above and beyond that, it requires someone familiar with detox from vaccine injuries—that is an entire workshop, not a simple answer.
Q: It’s been shown that DMSA, etc. provoking sends toxins all of the body, into joints, etc. Do you see this?
A: Not really. DMSA will bind metals in tissues. Because it is a sulfur bond, it is not easily reversible. The metal can be displaced by another metal with a higher affinity, so you can have some distribution. I also give DMSA according to the Cutler protocol—every three hours for three days every two weeks. I also make sure that patients have adequate glutathione and that they don’t have intestinal yeast. There is no way to remove metals without some distribution, but that is better (when managed properly) than leaving the metals in the body.
Mycotoxins: Considerations, Case Studies and Protocols
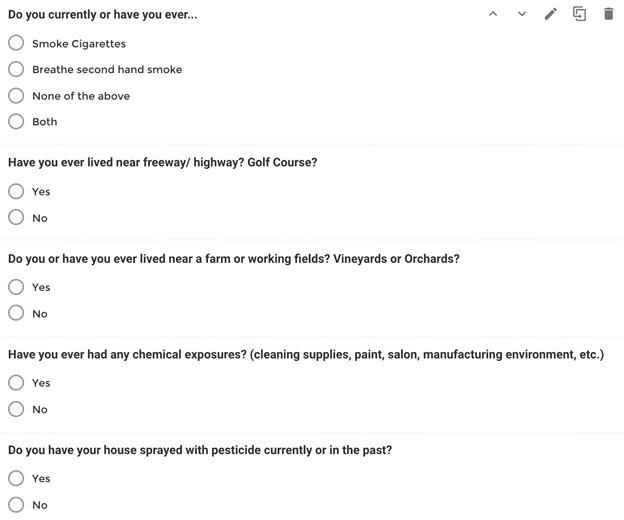
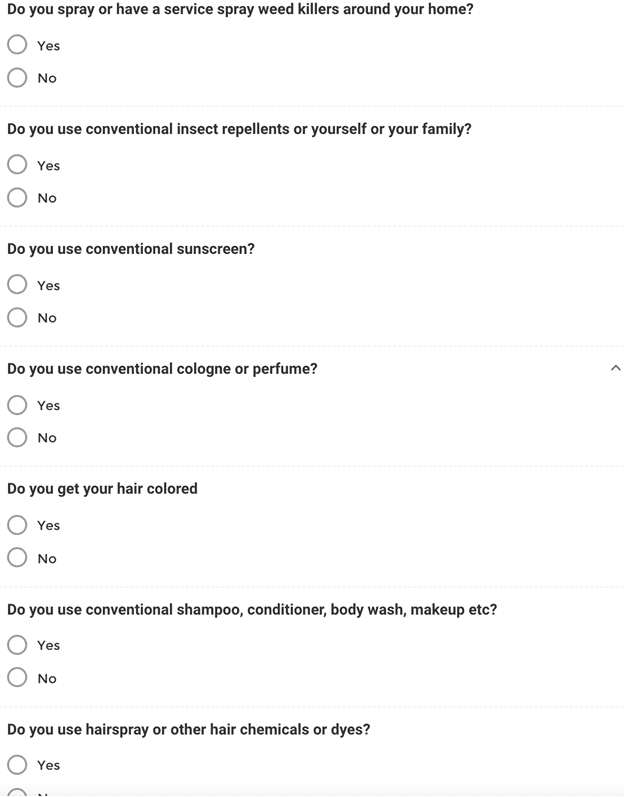
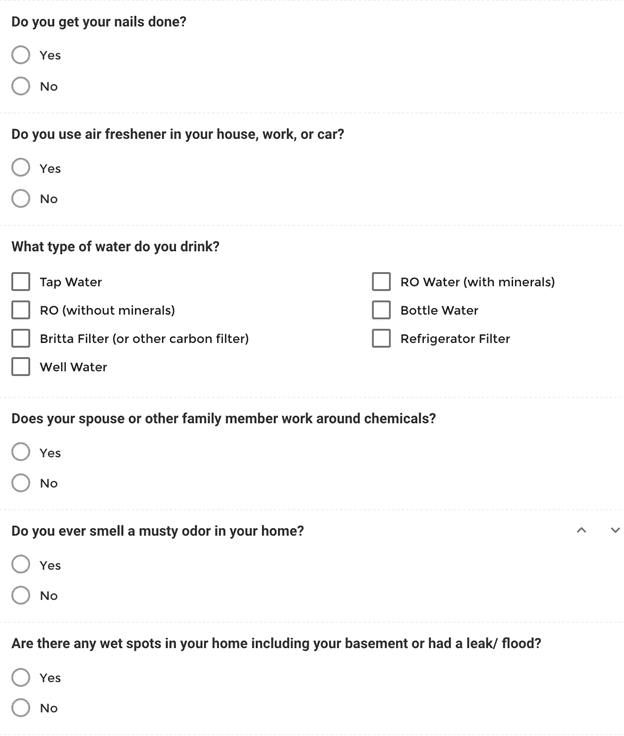
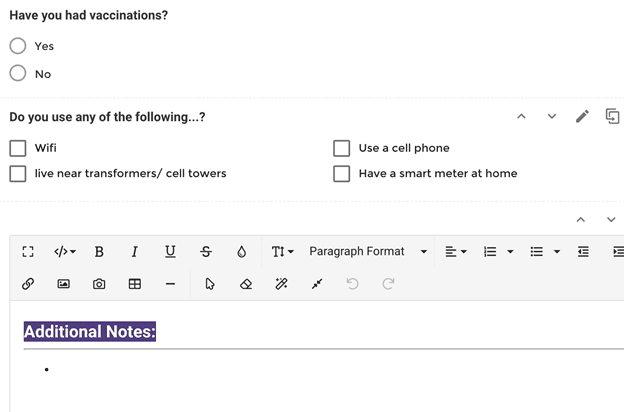
Q: Do you have a toxic exposure history form that you like?
A: The questions we ask in this area of our intake include the following. We also ask if they have any history of these exposures from their past.
Q: Would you be willing to share your symptom sheet and what you are utilizing for these patients to track symptoms?
A: Thank you for asking! Great question! We offer this and much more for our practitioners who go through our MHH certification program.
Q: What home mold testing do you recommend?
A: Home testing kits are not effective. We recommend our clients find a local mold testing company in their area to come out and test the house for mold. The price, depending on the state can range between $600-$800 for the testing and report.
Q: What do you use to break up the biofilm?
A: There are many different substances that can break up biofilm. The humic/fulvic compounds (like the ones found in the Cellcore product lines are effective at breaking up biofilm.
Biofilm X and Interphase are also great biofilm busters, as are coffee enemas, and Biocidin also breaks up biofilm. Keep in mind that biofilm, depending on how dense and how much build-up there is, can take as little as 8 weeks to as long as 8 months to fully break up and come out. I am basing this comment on our experience with our clients.
Q: Are you giving biofilm disrupters alongside the binders in your patients that had new molds show up in later tests, or do you think just using binders alone was lowering the load enough to allow the body to break up the biofilm on its own?
A: The protocols we put them on do break up biofilm, so it’s not common that we need to add something extra like Interphase or some added additional biofilm buster.
Q: Is the “chemical toxin” test the TOXDetect Profile®?
A: Yes.
Q: I do see a lot of sick patients that have high B12 lab readings. What are your thoughts on that?
A: Such a great question! They could be showing high levels of blood serum B12 or urinary metabolite patterns of high B12 for the following reasons:
- They are taking B12 currently.
- They have specific genetic methylation SNPS (MTRR A66G) that may be ‘mal expressing’ where they are not able to uptake the B12 into the cell … so they may show ‘high’ levels in blood serum or in urine, but are actually cellularly ‘deficient’ – in these cases either a sublingual or transdermal delivery method for methylated B12 is going to be the ideal delivery method for cellular uptake.
Q: Can you comment on when you choose Liposomal Glutathione vs N acetylcysteine for detox?
A: There are definitely varying opinions on this one. We actually use BOTH, glutathione, and NAC. Previously, a few years ago, we were using glutathione and saw marked improvements in homocysteine, CRP, and MCV numbers, which can indicate methylation issues, which can cause inefficiency of phase 1 AND 2 detox pathways, leading to excessive inflammation (of course we also had clients on methyl folate/methyl B12 as well, per their genetics — to make sure phase 1 and 2 Detox pathways were optimized). In the last year or so we have added NAC as well.
Q: I am interested in what exactly she is using for kidney/liver detox
A: We vary what we use from LVGB by DFH, to SP products, to Cellcore liver gallbladder support. There are many different brands that all work well.
Q: do you add in digestives like bile or HCL etc for support?
A: When we see it’s needed, yes we do. We definitely do when we are doing specific gut repair (after removing the toxins and confirming with labs) It’s a fine line when we are not wanting to overload the client with supplements. We want them to be able to take the least amount of supplements with the greatest effect. Too many supplements make the clients/patients feel overwhelmed and often they lose compliance.
Q: Please expand on biofilm treatment protocol… list options and when to use in the overall treatment protocol.
A: Discussed biofilm in the above questions.
Q: What is TUDCA and what is inside Para 1;2;3
A: Tudca provides liver/gallbladder support. You can go to HERE to see the labels on the Para’s.
Q: Do you see 3-4 week cough as a herx symptom?
A: I would ask more questions and get a deeper history on this. The client/patient may be having an IgG type of inflammatory reaction to an ingredient in one of the supplements that is causing the cough. Or it could be a recent food they recently started eating. More times than not, a herx is more ‘severe’ symptom wise, than a cough. So definitely ask more questions. You could also do an ‘elimination’ test by having them stop all supplements to see if the cough goes away, and then one at a time every 5 days or so, start adding in one more of the supplements on their list…. and record if sx comes back with one of the supplements.
Q: …But you are putting them on new supplements. So how do you tell the difference between a reaction and a herx?
A: It’s not as common to have a true ‘reaction’ to food/herb/nutraceutical based protocols. More than likely the sx are because the client is detoxing which can lead to mild sx or more severe ones (herx). If you are suspecting a true reaction, talk to the patient/client to get a history … they usually are already aware of their allergies to certain things. Use your discernment and if needed, take them off all supplements and slowly have them add one in at a time, sometimes micro dosing them with each supplement even. You’ll learn with experience!



